Unshrunk Resources
Welcome! If you’re here, you’re ready to take your next step– whether that means learning more, asking questions, exploring safer ways to taper off psychiatric drugs, or simply opening yourself up to the idea that a more vital, connected life awaits you or the person you care about.
My parents and I never had the information, resources, and support we needed to make meaningful choices about whether and how to engage with the diagnoses, medications, and therapies on offer from the American mental health industry. I put these basic resources together because they are what I wish we’d had so many years ago.
Only you can and should decide what’s right for you, whatever that might be. My hope is that these workbooks, FAQs, and learning resources I’ve shared below will be of use to you wherever you might be in your journey.
-Laura
Workbooks
I created these free workbooks as an offering to any of you facing a crossroads— whether you are currently taking psychiatric medications, you are a prescriber of psychiatric medications, or you’re a family member of someone on psych medications.

✨ For people currently taking psychiatric medications
Enter your email below to get this
FREE resource delivered to your inbox.

💊 For prescribers of psychiatric medications
Enter your email below to get this
FREE resource delivered to your inbox.
🏠 For family members of people on psychiatric medications
Enter your email below to get this
FREE resource delivered to your inbox.
Psychiatric Medication FAQs
-
SSRIs and other antidepressants
Antidepressants, including SSRIs, SNRIs, TCAs, and MAOIs, are known to cause a range of adverse effects, some more common than others. Frequently reported issues include emotional blunting, sexual dysfunction, weight changes, gastrointestinal disturbances like nausea or diarrhea, sleep disruptions, headaches, dizziness, and increased sweating.
Less common but more serious adverse effects include severe agitation or akathisia (a sense of inner restlessness), intense mood swings, heightened anxiety, or paradoxical reactions like increased suicidal thoughts, particularly in younger individuals. Some antidepressants can also affect cardiovascular function, contribute to serotonin syndrome when combined with other serotonergic drugs, or trigger manic episodes in those predisposed. In rare cases, long-term use has been associated with neurological symptoms like persistent movement disorders or protracted withdrawal effects after discontinuation.
AntipsychoticsAntipsychotics, both first-generation (typical) and second-generation (atypical), are associated with a range of adverse effects, some of which are more common and widely recognized. Frequently reported effects include sedation, weight gain, metabolic changes (such as increased blood sugar and cholesterol levels), dizziness, dry mouth, constipation, and movement-related symptoms like muscle stiffness or tremors. Many people also experience emotional dulling or cognitive slowing, which can affect daily functioning. Atypical antipsychotics, in particular, are known for their impact on metabolism, often leading to significant weight gain and an increased risk of diabetes.
More severe but less common effects include tardive dyskinesia (a potentially irreversible movement disorder characterized by involuntary facial and body movements), akathisia (a distressing inner restlessness that can be extreme), and neuroleptic malignant syndrome (a rare but life-threatening reaction involving fever, muscle rigidity, and autonomic instability). Some individuals experience extreme sedation, profound emotional detachment, or worsening cognitive issues over time. Additionally, long-term use has been linked to brain volume changes.
Mood stabilizersMood stabilizers, which are most commonly anticonvulsant drugs (such as valproate, lamotrigine, and carbamazepine) or lithium, come with a range of adverse effects that vary depending on the specific medication. Frequently reported effects include fatigue, dizziness, weight gain, gastrointestinal issues (such as nausea, diarrhea, or constipation), cognitive slowing or brain fog, and tremors. Some anticonvulsants can cause drowsiness or coordination problems, increasing the risk of falls or accidents. Lithium, in particular, requires regular blood monitoring due to its narrow therapeutic range and potential for toxicity, which can cause severe nausea, confusion, and muscle weakness.
Less common but more serious effects include severe skin reactions like Stevens-Johnson syndrome (most notably with lamotrigine), liver toxicity (especially with valproate), blood disorders (such as agranulocytosis with carbamazepine), and kidney or thyroid dysfunction with long-term lithium use. Some individuals experience significant cognitive impairment, emotional flattening, or worsening depressive symptoms over time.
StimulantsStimulants, commonly prescribed for attention-related difficulties, include medications like amphetamine-based drugs (e.g., Adderall, Vyvanse) and methylphenidate-based drugs (e.g., Ritalin, Concerta). Commonly reported adverse effects include increased heart rate, elevated blood pressure, reduced appetite, weight loss, insomnia, headaches, dry mouth, and gastrointestinal discomfort. Many people also experience heightened anxiety, jitteriness, or emotional ups and downs, especially as the drug wears off. Over time, some develop tolerance, requiring higher doses for the same effect, which can lead to dependency.
Less common but more severe adverse effects include cardiovascular complications (such as arrhythmias or increased risk of heart attack and stroke), psychiatric reactions like paranoia or hallucinations, and severe mood swings or aggression. Some individuals develop tics or movement disorders, and in rare cases, long-term use has been associated with cognitive impairments or changes in brain structure.
Anti-anxiety drugs
Anti-anxiety drugs, typically benzodiazepines (such as Xanax, Ativan, Klonopin, and Valium), come with a range of adverse effects. Commonly reported issues include drowsiness, dizziness, impaired coordination, memory problems, and cognitive slowing. Many people experience emotional numbing, reduced motivation, or difficulty concentrating. These drugs also depress the central nervous system, which can lead to slowed breathing and, in combination with alcohol or other sedatives, dangerous respiratory suppression. With continued use, tolerance develops, meaning higher doses may be needed for the same effect, increasing the risk of dependence.More severe but less common effects include paradoxical reactions such as increased agitation, aggression, or impulsivity. Long-term use is associated with cognitive decline, heightened anxiety between doses (interdose withdrawal), and a risk of developing protracted withdrawal symptoms that can last for months or years after stopping. Withdrawal from benzodiazepines, particularly after prolonged use, can be severe and include rebound anxiety, panic attacks, hallucinations, seizures, and in extreme cases, life-threatening withdrawal reactions. Due to these risks, sudden discontinuation is not recommended, and tapering should be done gradually.
Z-drugsZ-drugs, such as zolpidem (Ambien), eszopiclone (Lunesta), and zaleplon (Sonata), are commonly prescribed for sleep difficulties and share similarities with benzodiazepines in their effects. Commonly reported adverse effects include drowsiness, dizziness, memory issues, headaches, and next-day grogginess or cognitive fog. Some people experience unusual sleep behaviors, such as sleepwalking, sleep-eating, or even engaging in complex activities like driving without recollection. Dependence can develop with continued use, and stopping suddenly may lead to rebound insomnia, heightened anxiety, or other withdrawal symptoms.
Less common but more serious effects include hallucinations, extreme mood changes, and paradoxical reactions such as agitation or aggression. Some individuals experience severe cognitive impairment or blackouts, particularly when taking higher doses or combining Z-drugs with alcohol or other sedatives. Long-term use has been linked to an increased risk of falls, particularly in older adults, as well as potential neurodegenerative effects. Withdrawal from Z-drugs can include severe sleep disturbances, anxiety, tremors, and, in rare cases, seizures.
-
The most important place to start is the FDA-approved drug label. This official document, created by the drug manufacturer in collaboration with the FDA, provides essential information on approved uses, chemical properties, risks, interactions, and more. Unlike the short summaries often included with prescriptions, the full drug label is a detailed, professional document that can be 10-50 pages long. It includes crucial sections such as warnings, adverse reactions, dosage guidelines, and, in some cases, information about discontinuation effects. Even if your medication is prescribed for an “off-label” use, the drug label can still provide important insights to help you understand its potential effects and plan a safer taper if needed.
You can access the complete drug label online through official sources such as the DailyMed website (hosted by the U.S. National Library of Medicine) or the Drugs@FDA database. If you’re searching for your drug, use its full name—including both brand and generic names if applicable—and always check for the most up-to-date version of the label.
You can also access the FDA Adverse Event Reporting System (FAERS) Public Dashboard to search for any adverse events reported for your specific psychiatric drug. -
Many people feel helped by prescribed psychiatric medications– including antidepressants, mood stabilizers, benzodiazepines, stimulants, antipsychotics, and Z-drugs– especially when taken in the short term.
But many people don’t feel helped by psychiatric medications– and a certain percentage would go so far as to say they’ve been harmed by them. If you're considering tapering off psychiatric medication, you’re not alone. Many people reach a point where they wonder if they still need their medication, feel frustrated with side effects, or simply want to regain a sense of control over their well-being.
The decision to take or to come off a psychiatric drug is fundamentally personal– and risky. What’s right for one person is not right for someone else. Getting informed about the known risks and benefits of both taking and stopping these medications is essential when thinking through the right next steps.
-
If you’ve been taking psychiatric medication as prescribed, you might assume that stopping would be simple. After all, your doctor may not have warned you about potential difficulties, and you may have heard that these medications “aren’t addictive.” But it’s likely you might experience unexpected symptoms when trying to lower your dose or stop altogether. Many people are surprised to learn that psychiatric drugs can cause physical dependence, leading to withdrawal effects that can be challenging, sometimes even debilitating.
Psychiatric drug dependence isn’t the same as addiction. It happens when the body—especially the central nervous system—adjusts to the ongoing presence of a medication, making it difficult to stop without experiencing withdrawal. Symptoms can range from mild discomfort to severe physical and mental distress, and they’re often mistaken for a return of the original condition or the onset of a new one. Worse, many doctors are unaware of how to recognize or safely manage withdrawal, leaving people feeling confused and unsupported.
Feeling worse after stopping a medication is often seen by doctors, patients, and family members as proof that the med is necessary.
-
Psychiatric drug withdrawal is a deeply individual experience, with symptoms that can range from mild to severe, affecting mental, emotional, physical, cognitive, and sleep-related functioning. Two people taking the same medication for the same duration can have completely different withdrawal experiences, yet certain patterns have emerged. Some of the most commonly reported symptoms—especially after coming off medications too quickly—include difficulty concentrating, memory issues, heightened anxiety, panic attacks, paranoia, depression, rage, agitation, and intense fight-or-flight responses. Sleep disturbances, muscle pain, spasms, numbness or tingling, gastrointestinal issues, and the infamous “brain zaps” are also frequently mentioned. More severe symptoms, including convulsions, seizures, mania, hallucinations, or psychotic episodes have been documented both anecdotally and in drug label warnings.
Because withdrawal symptoms can mimic or even surpass what people originally sought help for, it’s not uncommon for them to be misinterpreted as relapse or the onset of a new psychiatric condition—often leading to more medications being prescribed. One of the biggest risk factors for severe withdrawal symptoms is reducing or stopping a drug too quickly. Those who experience this often go through different stages: Acute Withdrawal, where symptoms are most intense; Post-acute Withdrawal, where things become more manageable but can still be disruptive; and, for some, Protracted Withdrawal, where symptoms come and go unpredictably, sometimes triggered by stress, diet, illness, or other substances. This phase can be especially disorienting, as symptoms can persist or return even years after stopping the drug, making it difficult to recognize that what’s happening is still withdrawal.
-
Many people are surprised to learn that stopping a medication—even one taken exactly as prescribed—can cause withdrawal symptoms. They assume they would have been told this by their doctor prior to starting the medication, and that their doctor would have been well-versed in how to taper safely. But the reality is, most doctors receive little to no formal training in safe psychiatric drug tapering or managing symptoms of psychiatric drug withdrawal.
Medical education largely focuses on prescribing medications, not on how to help patients safely discontinue them. When withdrawal symptoms appear, many doctors mistake them for a relapse of the original condition or an emerging new disorder, rather than recognizing them as signs of the nervous system adjusting to the absence of the drug. This misunderstanding can lead to unhelpful or even harmful advice, such as increasing the dose again or adding new medications, rather than supporting a careful tapering process.
Even if your doctor isn’t fully informed about withdrawal, they can still be a valuable ally—but only if they respect your decision and are willing to learn alongside you. If a prescriber dismisses your concerns or discourages you from exploring a safe tapering plan, they may not be the right person to guide you through this journey. You deserve a doctor who listens, supports your goals, puts you in the driver’s seat of your taper, and prioritizes your well-being, even if that means acknowledging the limits of their own knowledge.
This is why self-education is so important. Understanding how psychiatric drugs affect your body and how to taper safely puts you in a stronger position to advocate for yourself. While your doctor’s guidance can be helpful, your best outcomes will come from combining informed medical supervision with your own informed decisions.
Tapering FAQs
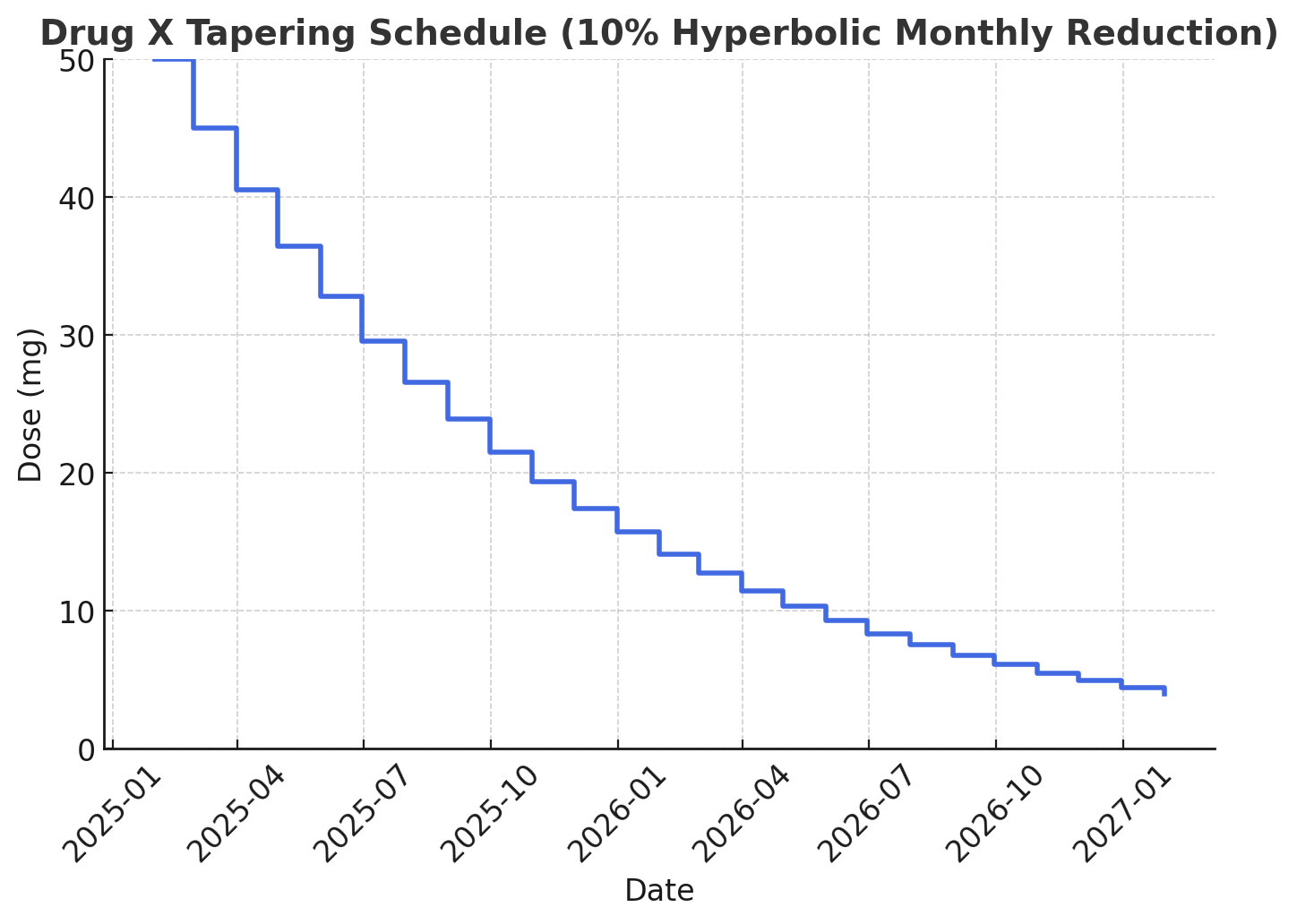

The psychiatric medication tapering schedule on the left— which shows the gradual reductions of a hyperbolic taper— is generally considered much safer than the harsh drop captured in the linear taper chart on the right. Keep reading to learn more.
-
Tapering off psychiatric medication means gradually reducing your dose over time rather than stopping suddenly. This process allows your brain and body to slowly adjust to the medication’s removal, reducing the risk of withdrawal symptoms that can be uncomfortable, disruptive, or even debilitating– and that can last for months or even years.
Using psychiatric medications regularly for any length of time can alter the structure and function of the central nervous system in profound ways. An abrupt or poorly planned taper can lead to intense withdrawal effects that are often mistaken for relapse.
However, tapering as safely and successfully as possible is about much more than just cutting down on your dose—it requires careful preparation, an assessment of your current circumstances, lots of reflection, and a strategic plan to support your nervous system through the transition.
Just as important as the taper itself is the knowledge you gain beforehand. It can make a world of difference to spent time in advance of your taper:
Understanding how your medication affects your body
Learning how to taper off your medication as safely as possible
Getting clear on the nature of psychiatric drug withdrawal so that you learn how to recognize potential withdrawal symptoms
Generally speaking, doctors are not trained in how to taper patients properly off medications or even how to recognize psychiatric drug withdrawal, so taking the time to educate yourself can help you advocate for a safer and more successful tapering process.
-
You may have heard that it’s important to “go slow” when tapering off an SSRI, anti-anxiety drug, mood stabilizer, antipsychotic, or other psychiatric medication, but what does that actually mean? And how slow is slow enough to minimize the risk of experiencing difficult withdrawal symptoms?
Everyone is different, and there is no one right answer to this question– but generally speaking, a reduction rate of somewhere between 5-10% per month– with that amount calculated as a percentage of the previous month’s dose, not the original starting dose– seems to be what yields the smoothest outcomes for most people most of the time. This approach is called hyperbolic tapering, because the reduction amount is getting progressively smaller over time.
Though this means a much longer time spent tapering than simply reducing the same amount each month– which is called linear tapering– this hyperbolic approach dramatically reduces the risk of painful and disabling withdrawal symptoms, increasing your chances of successfully getting off medication and staying off for the longer term.
To see what hyperbolic vs. linear tapering looks like, check out the graphs above.
You can see how much gentler and subtler the hyperbolic tapering schedule is– and also, that it takes much longer. Once you’ve decided that you want to stop taking medication, the desire to be done can feel overwhelming. The idea of stretching out the process over months (or even years) might seem frustrating or unnecessary. But here’s the reality: coming off psychiatric drugs too quickly can trigger severe and long-lasting withdrawal symptoms. For a certain percentage of people, these withdrawal problems can last for months or even years. Many doctors aren’t trained to recognize withdrawal, leaving people feeling confused, unsupported, and even worse than before.A thoughtful, informed approach helps ensure a smoother experience, giving your body the time it needs to recalibrate to the growing absence of medication it’s been grown physiologically dependent on over time.
-
Inner Compass Initiative, the non-profit organization that I founded in 2018, is stockpiled with tons of free information and resources for the psychiatric drug tapering and withdrawal journey— including a step-by-step, self-directed tapering manual.

